
In this blog, three Cochrane ReviewCochrane Reviews are systematic reviews. In systematic reviews we search for and summarize studies that answer a specific research question (e.g. is paracetamol effective and safe for treating back pain?). The studies are identified, assessed, and summarized by using a systematic and predefined approach. They inform recommendations for healthcare and research. authors share the latest evidence on dressings and topical agents for pressure ulcers. Using a technique (network meta-analysisThe use of statistical techniques in a systematic review to combine the results of included studies. Sometimes misused as a synonym for systematic reviews, where the review includes a meta-analysis. ) to compare each treatmentSomething done with the aim of improving health or relieving suffering. For example, medicines, surgery, psychological and physical therapies, diet and exercise changes. with every other in the trialsClinical trials are research studies involving people who use healthcare services. They often compare a new or different treatment with the best treatment currently available. This is to test whether the new or different treatment is safe, effective and any better than what is currently used. No matter how promising a new treatment may appear during tests in a laboratory, it must go through clinical trials before its benefits and risks can really be known., are we any further forward in making informed choices about which to use?
Page last checked 15 March 2023. You can find all our blogs on Pressure ulcers from the page Pressure ulcers (pressure injuries): evidence and resources.
We set out to answer this question by doing a systematic reviewIn systematic reviews we search for and summarize studies that answer a specific research question (e.g. is paracetamol effective and safe for treating back pain?). The studies are identified, assessed, and summarized by using a systematic and predefined approach. They inform recommendations for healthcare and research. and meta-analysis of the evidence on dressings and topical agents for healing pressure ulcers. The result is a Cochrane Review, Dressings and topical agents for treating pressure ulcers (published February 2017). We think we have done a good review – but it is dealing with poor quality evidence, and because of that, there is a lot of uncertainty about the results.
A confusing picture
There are many dressing and topical treatments for pressure ulcers, with variation within those treatments, e.g. dressings for wounds with different levels of exudate. Some of these treatments have been investigated in trials over the past 30-40 years, but we don’t know which treatments are the best in terms of wound healing. Clinical guidelines (e.g. NICE in the UK) have recommended that saline gauze should not be used as a treatment for pressure ulcers, but do not give guidance regarding which, if any, dressing or topical agent might be most effective.
It’s a confusing picture that is not really helped by looking at the evidence from individual trials. Firstly trials are often small and conclusions are vague. Secondly although it is useful to some extent to learn that dressing 1 is more likely to heal a pressure ulcer than dressing 2, and dressing 3 is better than dressing 4, etc, how do we decide which is the best overall? This is particularly difficult when not all these dressings have been compared with each other in trials.
Network meta-analysis (NMA)
In order to deal with this confusing array of evidence about dressings and topical agents, we used network meta-analysis: this allows us to combine the results of multiple trials comparing different treatments, forming a network linked by common comparators. The value of this approach is that it maintains the randomisationRandomization is the process of randomly dividing into groups the people taking part in a trial. One group (the intervention group) will be given the intervention being tested (for example a drug, surgery, or exercise) and compared with a group which does not receive the intervention (the control group). of the original trials but allows us to compare treatments indirectly that have not been compared directly in trials. As with standard meta-analysis, a number of assumptions must be met, especially around the meaningful pooling of dataData is the information collected through research. from studies with potentially different studyAn investigation of a healthcare problem. There are different types of studies used to answer research questions, for example randomised controlled trials or observational studies. populations and approaches.
The NMA process allows us to compare each treatment with every other in the network, and has the added benefit of providing a ranked order of treatments in the network in terms of the treatment most likely to be the best (for the given outcomeOutcomes are measures of health (for example quality of life, pain, blood sugar levels) that can be used to assess the effectiveness and safety of a treatment or other intervention (for example a drug, surgery, or exercise). In research, the outcomes considered most important are ‘primary outcomes’ and those considered less important are ‘secondary outcomes’.), followed by the next best and so on.
As with other evidence synthesis, it is also important to assess the quality (or the certainty of the evidenceThe certainty (or quality) of evidence is the extent to which we can be confident that what the research tells us about a particular treatment effect is likely to be accurate. Concerns about factors such as bias can reduce the certainty of the evidence. Evidence may be of high certainty; moderate certainty; low certainty or very-low certainty. Cochrane has adopted the GRADE approach (Grading of Recommendations Assessment, Development and Evaluation) for assessing certainty (or quality) of evidence. Find out more here: https://training.cochrane.org/grade-approach) in a network meta-analysis. This can be done using a modified version of the GRADE approach.
NMA of treatments for healing pressure ulcers
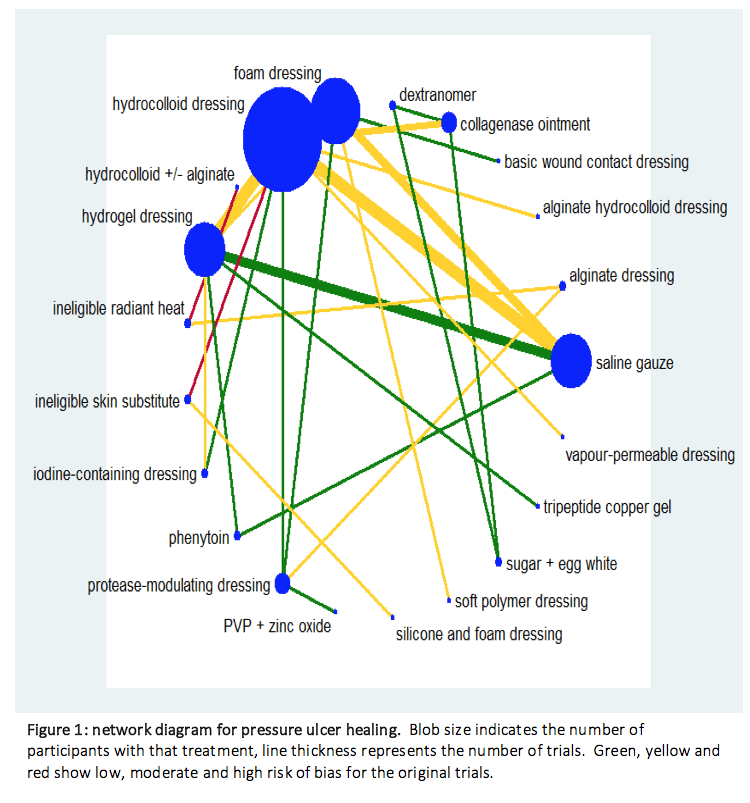
We found 51 randomized trials, and 39 could be linked to form a network joining 21 treatments in about 3000 participants (see the network diagram below, which shows the evidence from trials). There were 13 different dressings and 6 topical agents and 2 other linking interventions (we only included topical agents that could be left on the wound, so not washes or irrigating fluids).
We got results for 210 comparisons covering every pair of treatments and were also able to obtain the rank order of treatments (along with probabilities that each treatment is the best, the next best, and so on).
To make interpretation easier, we focused on the results for the 20 comparisons with saline gauze, and the rank order of all the treatments in the network for healing.
What does NMA tell us that we didn’t know before?
Unfortunately, nearly all of the evidence was low or very low quality – and that was mainly because many of the original trials were poorly conducted and, in the network, there weren’t many participants for the number of treatments considered. Low quality means we only have limited confidence in the overall effect (result): ‘the true effect may be substantially different from the estimate of the effect’ (Balshelm, 2011). ‘Very low quality’ loosely translates as ‘we can’t trust the results’.
Consequently, we are unable to determine which dressings or topical agents are the most likely to heal pressure ulcers, and it is mostly unclear whether the treatments examined are more effective than saline gauze (which, in the trials, had a median healing rateThe speed or frequency of occurrence of an event, usually expressed with respect to time. For instance, a mortality rate might be the number of deaths per year, per 100,000 people. of 150 per 1000). What we can say is that protease-modulating dressings, foam dressings or collagenase ointment may be better at healing than gauze; but even this evidence is not certain enough to be an adequate guide for treatment choices. Further information for all the comparisons is in the review. The very low quality of the evidence as a whole means we can’t give meaningful information on which treatment had the probability of being best, that is, to rank the treatments.
What next?
Now, having uncertain evidence is all very well in academic research – it just means we need more research. But how does it help nurses to make decisions today (not in 2, 5, 10 years’ time)? If they want to know about which treatment to use, then what do they do? How do we all deal with uncertainty?
When there is uncertainty, we believe it is important for nurses to have the evidence to hand as a basis for decision making, being fully aware of its limitations, and using their clinical judgment about the different treatments to consolidate (or reject) the uncertain evidence described here. It is important also to bring in other factors (ease of use, cost, patient preference, etc). We need to work with, rather than independently of, the evidence.
If the evidence quality had been better, the review would probably have informed updates of guidelines. What we can say is that this extensive Cochrane Review does not contradict the NICE 2014 guideline recommendations, which are (for adults): not to use saline gauze (in the UK), and – for other dressings – to discuss with adults the type of dressing, taking into account pain and tolerance, position of the ulcer, amount of exudate and frequency of dressing change.
It would have been good to have some definitive answers to the questions – but we can’t make a silk purse out of a sow’s ear. Instead, we all have to do the best we can with what we’ve got. The evidence is pretty poor, but, in partnership with clinical experience and discussion with the patient, it can become much more valuable.
References may be found here.
Join in the conversation on Twitter with @CochraneUK @CochraneWounds #EENursing or leave a comment on the blog.
Disclosure of interest: Dr Westby discloses a grant from NIHR (UK) and reports her work on the 2014 NICE clinical guidelineA systematically developed statement for practitioners and participants about appropriate health care for specific clinical circumstances. on pressure ulcers. Dr. Dumville discloses a grant from NIHR (UK). Dr. Norman reports grants from NIHR (UK), during the conduct of the study.